What clinically significant symptoms does Kelly display in regard to eating and shape? What eating disorder encapsulates these symptoms?
DSM Diagnosis
307.51 Binge-Eating Disorder, Moderate
296.20 Major Depressive Disorder, Single Episode, Mild
Pregnancy (six weeks)
995.81 Spouse or Partner Violence
995.82 Spouse or Partner Abuse, Psychological
V60.2 Low Income
V62.89 Phase of Life Problem
Rationale
Kelly met the criteria for Binge Eating Disorder as follows:
A. She reports recurrent episodes of binge eating.
B. The episodes are characterized by (three symptoms are necessary):
1. Kelly eats large amounts of food even when not physically hungry.
2. She eats alone because she is embarrassed at how much she eats.
3. She feels disgusted with herself, depressed, and guilty after overeating.
C. Kelly experiences marked distress (depressed, out of control) regarding the binge eating.
D. The binge eating has occurred every other day for years.
E. Although Kelly reports that she uses laxatives about once every two weeks, the binges are not regularly associated with laxative use. For the last six weeks, she has used an emetic, but whether that is to harm her fetus or to compensate for binges is unknown.
The specifier “moderate” is used because Kelly reports bingeing every other day, which puts her at about four binges per week.
Kelly also meets the following symptoms for Major Depressive Disorder:
1. She reports depressed mood and was tearful in the initial therapy session.
2. She has experienced a loss of interest in maintaining personal hygiene (hair was unwashed and uncombed, and sweatshirt was worn inside out when she came to initial session).
3. Kelly has experienced significant weight gain and increased appetite (which could also be ascribed to the eating disorder and/or the pregnancy).
4. She has feelings of worthlessness and shame over eating disorder and failed marriage.
5. Kelly has a diminished ability to think or indecisiveness in that she can find no other way to cope with an unwanted pregnancy other than to damage the fetus through blows to the stomach and using an emetic after binges. She also cannot plan for how to end her marriage and financially support herself.
6. There has been a suicide attempt in the past six weeks and current feelings of suicide.
The specifier “single episode” has been given because we have no evidence that Kelly has suffered from an episode in the past. “Mild” has been assigned because she definitively only meets five symptoms of depression.
Several V Codes have also been added to capture the aspects of Kelly’s life that are particularly problematic. The first is Spouse or Partner Violence, Physical. Although Kelly seems reluctant to speak of this, she says that her husband has shoved and pushed her around. The additional V code of Spouse or Partner Abuse, Psychological was added because she says he is verbally abusive of her, calling her “fat” and “lazy.” Low Income is another V code added since Kelly says she has no money to be able to get a divorce, and she has no income coming in. A Phase of Life problem represents the fact that she seems at a loss of what to do after finishing graduate school, and she has extreme aversion to the pregnancy.
Treatment
A priority for intervention is to develop a safety contract for Kelly, to see if she is able to commit to keeping herself safe. If she is unable to do that, she might have to be hospitalized to ensure her safety and that of the fetus.
A medical evaluation is important to see if Kelly has experienced any health risks from being overweight, and if she has caused harm to her fetus. A physical examination and/or blood tests to determine electrolytes would be important to discover if there has been any effects from laxative use or the recent use of emetics.
Intervention also needs to address Kelly’s options for her pregnancy. She could be referred to a Planned Parenthood agency to discuss alternatives. She could also be provided with a referral for Legal Aid for help with the divorce and possible child support.
Since Kelly has already had a course of cognitive-behavioral treatment and psychodynamically oriented treatment, she could be offered Dialetical Behavioral Therapy (DBT), a promising intervention for Binge Eating Disorder (Wilson, 2005). A primary goal of DBT, which is an intensive treatment, is to teach people “how to use mindfulness and emotion regulation skills to cope with negative affect without resorting to binge eating” (Wilson, 2005). Finally, if Kelly benefited from Overeaters Anonymous in the past, she could be referred to groups in the area for needed social support.
A psychiatric evaluation might be indicated for Kelly. Given her depression and suicidality, she might benefit from a course of antidepressants. However, if she continues with the pregnancy, the risk/benefits of such a course will have to be evaluated.
Critical Perspective
One of the main critiques of the DSM is the increasing trend for “normal” behaviors to be defined as mental disorders, thus furthering the interests of the psychiatric community and the pharmaceutical companies (Kutchins & Kirk, 1997). This critique could also be applied to Binge Eating Disorder, which has been adopted into the DSM-5. The argument could be made that since one-third of the U.S. population are overweight and another third are obese (National Institute of Diabetes and Digestive and Kidney Diseases, 2007), this represents a “normal” state for people in the U.S. Although of course not all overweight and obese people are binge eaters (and people of normal weight can be binge eaters), many are, which may qualify them for the diagnosis of Binge Eating Disorder.
Another side of the argument, however, is illustrated in the case study of “Kelly,” which shows the anguish and level of impairment that may be associated with Binge Eating Disorder. The National Co-Morbidity Replication Survey indicated that Binge Eating Disorder is not only more common than either anorexia or bulimia, it is also associated with high co-morbidity with other disorders, which adds support to the case that it should belong in the DSM as a recognized disorder (Hudson et al., 2006). As a result, clinicians will be more apt to screen for the disorder and to refer for appropriate treatment. This is important given the level of suffering and the associated health risks with Binge Eating Disorder.
Kelly has a history of binge eating from a young age and feels like she cannot control her eating. Her mood and self-esteem suffer as a result. Her weight – at 200 pounds - is excessive for her height (five foot six inches). She admits to occasional (every two weeks) laxative use. Given the out of control nature of her binges and the way she feels afterward, Kelly seems to meet the criteria for Binge-Eating Disorder.
You might also like to view...
How many respondents reported feeling “Pretty Happy” or better with their marriage?
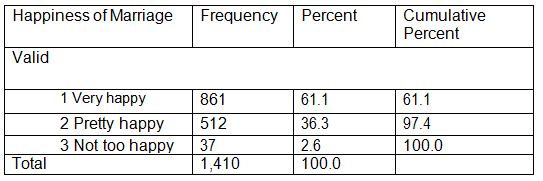
A. 61.1
B. 512
C. 861
D. 1,373
One major thing that human service workers who come in contact with persons with HIV/AIDS will have to be aware of and learn to deal with is:
a. The ridicule they may get from other professionals. b. There own fears and anxieties about getting the disease. c. The rules for safe engagement. d. Latex glove allergies.
Your text claims that averages are found everywhere: school, sports, and climate issues. Name an example not discussed in your text where you would use statistics; explain which central tendency(ies) you would use and why.
What will be an ideal response?
Explain the effect that outliers have on mean.
What will be an ideal response?